
That gap — between deployment speed and governance readiness — is where compliance exposure lives.
AI agents are not standard software. They act autonomously, call external tools, access EHR data, hand off context to other agents, and make decisions that affect patients. Every one of those actions is a potential compliance event. Traditional healthcare security frameworks were built around human access to data, not autonomous systems with dynamic tool-calling authority.
This guide covers the regulatory frameworks that apply, the specific compliance risks that agentic architecture introduces, what you need to build in during development, and why runtime enforcement is the layer most teams leave out entirely.
Key Takeaways
- Six regulatory frameworks apply to healthcare AI agents — HIPAA, HITECH, FDA CDS guidance, 21 CFR Part 11, GDPR, and the EU AI Act — with no carve-out because a model acted instead of a person
- Prompt injection, retrieval poisoning, and multi-agent handoffs are compliance risks, not just security ones; each can trigger a HIPAA violation
- Two layers of compliance are required: design decisions made during development and runtime enforcement on every inference and action
- Audit trails need decision-level evidence: which agent, which data, what action, and what authorization — session logs alone don't satisfy regulators
- Post-deployment monitoring is a compliance obligation; production behavior drifts, and undetected drift becomes regulatory exposure
The Regulatory Landscape Healthcare AI Agents Must Navigate
Healthcare AI doesn't exist in a regulatory vacuum. Multiple frameworks apply simultaneously, and none of them reduce their requirements because the actor is an AI system rather than a human clinician.
HIPAA and HITECH
Under 45 CFR §164.312(a)(1), technical policies must allow access to ePHI only to persons or software programs granted access rights. That language directly includes AI agents. The same access controls, minimum necessary restrictions, encryption standards, and audit trail requirements that govern a nurse's EHR login govern an AI agent's EHR query.
The audit controls standard at §164.312(b) requires mechanisms that "record and examine activity in information systems that contain or use electronic protected health information." Absent audit records are themselves a violation — separate from any underlying incident.
AI vendors that process ePHI on behalf of a covered entity are business associates. They require HIPAA-compliant Business Associate Agreements regardless of other certifications they hold.
FDA Clinical Decision Support Classification
The FDA's 2022 CDS guidance draws a line that every team building clinical AI agents must understand. Non-device CDS presents analysis for independent clinician review — the clinician can examine the basis for the recommendation and decide independently. Device software makes autonomous or effectively unreviewable decisions.
Agents that perform autonomous patient triage, route cases based on risk scores, or flag results for automated follow-up without surfacing their reasoning for clinician review sit on the device side of that line. Misclassifying them as non-device CDS creates both regulatory liability and patient safety risk.
21 CFR Part 11 and GxP Environments
For AI agents operating in clinical trial, pharmaceutical manufacturing, or medical device development contexts, 21 CFR Part 11 applies to electronic records the agent creates, modifies, or transmits. Requirements include:
- Demonstrate accuracy, reliability, and consistent intended performance through formal validation
- Restrict system access to authorized individuals only
- Maintain secure, computer-generated, time-stamped audit trails that cannot obscure prior entries
The specific challenge AI creates for Computer System Validation is behavioral drift — an agent may shift outputs as it processes new data without a formal code change triggering re-validation. Organizations must define upfront what constitutes a change that requires re-validation.
GDPR, EHDS, and the EU AI Act
For organizations handling EU patient data, three frameworks stack on top of each other:
- GDPR Article 9 places health data in a special category with heightened processing restrictions
- GDPR Article 35 mandates a Data Protection Impact Assessment before high-risk processing; large-scale health data processing triggers this requirement automatically
- GDPR Article 22 gives patients the right not to be subject to decisions made solely through automated processing that significantly affects them
- EHDS Regulation (EU) 2025/327 requires data permits from health data access bodies for any secondary use of EU health data, including AI training
- EU AI Act (EU) 2024/1689 classifies emergency triage and safety-critical clinical AI as high-risk, triggering mandatory risk management, human oversight, logging, and post-market monitoring obligations

ONC Transparency Requirements
Back in the US, ONC's HTI-1 final rule, finalized in January 2024, established the first transparency requirements for AI and predictive algorithms embedded in certified health IT. Covered systems must support documentation of decision support interventions, including the evidence base, risk management information, and limitations of predictive models.
For development teams, this means AI governance documentation is now a condition of program participation in federally funded environments — not an optional deliverable to address post-launch.
Where Agentic AI Creates New Compliance Risks
Standard compliance frameworks were designed around human access to data. Agentic AI introduces a different threat model — one where the system itself is the actor, with autonomous authority to retrieve data, call tools, and hand off context to other agents.
Attack Surfaces That Are Also Compliance Surfaces
NIST identified in January 2025 that many AI agents are vulnerable to "agent hijacking" — indirect prompt injection where attackers insert malicious instructions into data the agent later consumes. The OWASP LLM Top 10 for 2025 maps the specific risks:
- LLM01 Prompt Injection: Adversarial inputs that hijack agent behavior mid-workflow
- LLM04 Data and Model Poisoning: Corrupting the training data or knowledge base agents rely on
- LLM06 Excessive Agency: Agents with overly broad permissions executing actions beyond their intended scope
- LLM08 Vector and Embedding Weaknesses: RAG systems vulnerable to hidden-text poisoning and cross-context information leakage

Each of these is not just a security incident when PHI is involved — it's a potential HIPAA violation.
The Minimum Necessary Gap
A human clinician naturally limits their data access by clinical context. An AI agent with broad EHR permissions may technically reach far more PHI than any individual task requires. HIPAA's minimum necessary standard requires reasonable efforts to limit PHI access to what's needed for the intended purpose.
For AI agents, satisfying this standard requires attribute-based access control enforced at the operation level — not just role-level permissions assigned at provisioning. An agent should only be able to retrieve the specific fields its current task requires, not everything its role technically permits.
Multi-Agent Handoff Risks
In systems where agents pass context, data, or authority to other agents, three specific compliance risks emerge:
- PHI crosses boundaries without explicit human authorization at each transfer
- Audit trails break at handoff points if the receiving system doesn't inherit the logging context
- Scope escalates when the receiving agent has broader permissions than the initiating agent intended to delegate
No established framework covers agent-to-agent data transfers in healthcare IT — organizations must build these controls themselves.
Data Spillage and Compliance Drift
Without strict session isolation, an agent handling one patient interaction can carry PHI into a subsequent session. In high-throughput environments processing dozens of concurrent sessions, a single gap in isolation can affect multiple patients simultaneously.
Beyond spillage, there's a subtler risk: compliance drift. An agent that passes pre-deployment testing may behave differently in production as it encounters edge cases, adversarial inputs, or data distributions missing from test environments. Unlike traditional software, agents can produce non-deterministic outputs that deviate from compliant behavior without any code change. Regulators won't accept "the model changed" as an explanation — post-deployment monitoring is a compliance obligation.
Building Compliance In: Development-Phase Requirements
Architecture decisions made during development set the ceiling for what compliance can actually achieve at runtime. Teams that defer these choices inherit technical debt that regulators don't forgive.
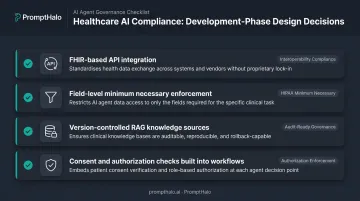
Design Choices With Compliance Consequences
- Use FHIR-based APIs for EHR integration rather than broad database access — this enforces query-level boundaries rather than schema-level access
- Enforce minimum necessary at the field level in data pipelines, not just at the system access layer
- Version-control RAG knowledge sources and restrict retrieval to vetted, approved content — open retrieval against uncontrolled sources creates both hallucination and poisoning risk
- Build consent and authorization checks into agent workflows before any PHI is accessed, not as an afterthought
FDA Classification as a Development Prerequisite
The CDS classification decision should happen before clinical deployment, not after. Teams need to:
- Classification rationale: document exactly what each agent does and doesn't do autonomously, with enough specificity to defend the boundary
- Judgment boundary: define precisely where the agent informs versus replaces clinician decision-making in your specific deployment
- Review interface: give clinicians a way to genuinely interrogate the recommendation basis — not just accept or override a black-box output
If the basis for a recommendation cannot be surfaced for independent review, the system is likely operating as an unlicensed medical device.
BAA Requirements in the Development Context
Every AI vendor, model provider, or cloud service that will process ePHI — including during development and testing — must execute a HIPAA-compliant BAA before any PHI flows to their systems. HHS is explicit that cloud service providers handling ePHI are business associates even if the data is encrypted and the provider cannot view it.
This gate belongs in the vendor assessment process before architecture decisions are finalized. Vendors that won't execute BAAs cannot be used in PHI-touching workflows, regardless of other certifications they hold.
Agent Permission Scoping
During development, each agent should be scoped to the minimum authority required for its defined function. Specifically:
- Agents should not inherit permissions through multi-agent interactions
- Agents should not be able to escalate their own access mid-task
- Human-in-the-loop checkpoints should be designed into workflows before agents execute high-stakes actions — particularly in clinical decision support, billing, and patient communication
Runtime Enforcement: Why Build-Time Compliance Isn't Enough
Development-phase compliance addresses what an agent is designed to do. Production environments expose agents to adversarial inputs, unexpected data, and interaction patterns that testing cannot fully anticipate.
Runtime enforcement (evaluating and controlling every agent action at the moment of execution) is the necessary second layer.
What Runtime Enforcement Must Cover
For healthcare AI, runtime controls need to address:
- Prompt injection and jailbreak blocking before adversarial inputs cause PHI exposure or unauthorized agent actions
- Out-of-scope tool and API call enforcement so agents cannot interact with systems beyond their defined authority
- Retrieval poisoning containment to prevent manipulated content from corrupting clinical decision support outputs
- Session isolation to prevent PHI from one patient interaction bleeding into another
Authority Decay Across Multi-Agent Workflows
Authority decay is a core runtime requirement for agentic systems: an agent's permissions should shrink, not persist unchanged, as a workflow branches into sub-tasks or hands off to other agents.
PromptHalo's Runtime Security solution addresses this through agent security passports that travel with each request, with policy, budget, and authority decay built into the passport structure. Authority is scoped per action and enforced externally, so an agent cannot grant itself more access than it was initially given. Budgets decay across three dimensions — time, steps, and risk — and re-authorization is required when any threshold is exceeded.
This is particularly relevant in healthcare: an agent that initiates a workflow with appropriate EHR permissions should not carry those permissions into downstream sub-agents that don't require them. PromptHalo sits inline on every inference, tool call, and agent-to-agent handoff — deciding allow, restrict, challenge, deny, or monitor in under 100ms, without touching the underlying model.
Audit Trails and Evidence Generation for Regulatory Reporting
What HIPAA Actually Requires for AI Agents
The §164.312(b) audit controls standard requires mechanisms to "record and examine activity in information systems that contain or use electronic protected health information." For AI agents, session-level logs showing that a tool was used are not sufficient.
Compliant audit trails for AI agents must capture:
- Which agent accessed which ePHI fields
- What action it took and what data sources it drew on
- What reasoning or recommendation it produced
- What human or system authorization governed the workflow
OCR examiners requesting audit evidence for an AI-related incident will ask for this level of detail. Absent records are themselves a violation.
Explainability as a Compliance Requirement
In clinical contexts, audit logs must provide a human-readable rationale that a clinician or compliance reviewer can evaluate and challenge. This requirement intersects directly with FDA CDS classification: if the system cannot surface the basis for a clinical recommendation for independent review, it risks classification as an unlicensed medical device.
Technical Standards for Compliant Audit Infrastructure
Explainability requirements don't exist in isolation — the infrastructure behind them must meet its own regulatory bar. For GxP environments, 21 CFR Part 11 mandates that audit trails be:
- Secure, computer-generated, and time-stamped
- Structured so prior entries cannot be obscured or overwritten
- Retained at least as long as the subject records
- Available for agency review on demand
PromptHalo's audit logs are append-only and tamper-evident: once an event is written, it cannot be modified or removed. Each entry captures the decision rationale, the acting agent's identity, session and tenant context, and a timestamp — creating a replayable evidence trail suited for compliance export and post-incident investigation.
Audit infrastructure also needs to feed organizational SIEM systems so that PHI access patterns by AI agents are visible to security teams alongside human access monitoring — not siloed in a separate tool that compliance reviewers have to check independently.
Frequently Asked Questions
What are the compliance requirements for AI agents in healthcare?
Healthcare AI agents must satisfy HIPAA and HITECH for any ePHI access — including access controls, minimum necessary restrictions, encryption, and audit trails. FDA CDS guidance applies to clinical decision support, 21 CFR Part 11 governs agents in FDA-regulated environments, and GDPR/EHDS obligations apply for EU patient data. Every framework applies at full force regardless of whether the actor is human or AI.
How is AI used in healthcare compliance?
Healthcare AI plays two distinct roles. As compliance tools, agents monitor access patterns, detect anomalies, and generate audit documentation at scale. As regulated entities, clinical, billing, and administrative agents must themselves comply with HIPAA, FDA, and other frameworks in how they access and act on patient data.
Does HIPAA apply to AI systems that access patient records?
Yes, without exception. Under 45 CFR §164.312, access control requirements explicitly apply to "software programs" granted access rights, not just human users. AI vendors processing ePHI on a covered entity's behalf are business associates and require BAAs — this includes cloud providers and model API providers.
What is the FDA's classification for AI used in clinical decision support?
The 2022 FDA CDS guidance distinguishes non-device software (presenting analysis for independent clinician review) from device software (making autonomous or effectively unreviewable decisions). Agents that route patients, flag results for automated action, or recommend treatment without surfacing their reasoning for clinician review typically meet device criteria and require FDA premarket review.
How do you build audit trails into a healthcare AI agent?
Compliant audit trails must capture operation-level evidence for every agent action: which data was accessed, what the agent did, and what authorization governed the workflow. Logs must be tamper-evident and meet HIPAA §164.312(b) audit controls — and 21 CFR Part 11 requirements where FDA-regulated workflows are involved.
What are the biggest compliance risks specific to agentic AI in healthcare?
Agentic systems introduce compliance risks that traditional tools weren't built to catch:
- Prompt injection and jailbreaks causing PHI leakage or unauthorized actions
- Minimum necessary violations from overly broad agent permissions
- Audit trail gaps at multi-agent handoff points
- Data spillage across patient sessions
- Compliance drift — non-compliant outputs appearing in production without any code change triggering re-evaluation


